The following excerpt is taken from The Physiology of EFM, a PeriGen white paper written by Emily Hamilton, MDCM and Philip Warrick, Ph.D. Its contents are among the topics to be covered at the free March 16th lunchtime labor & delivery training webinar.
Click Here to Register | Space is Filling Fast
[fruitful_sep]
Late Fetal Heart Rate (FHR) Decelerations
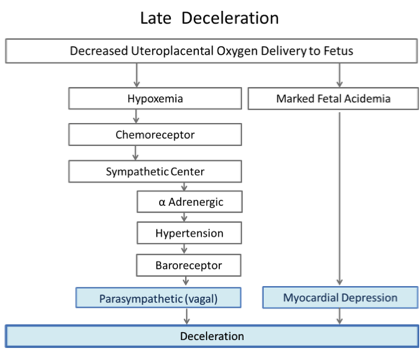
Figure 3: Two pathways are involved with late decelerations, adapted from Martin 1979 (1) and Freeman et al. (2)
To simulate decreased uteroplacental oxygen delivery, Martin applied repeated hypogastric artery occlusions in sheep. These occlusions resulted in fetal hypertension which was followed by vagally mediated decelerations. The degree of hypertension and the amount of deceleration were closely related, although some deceleration remained when the transient hypertension was prevented by alpha-adrenergic blockade. The timing of the onset, nadir and end of the deceleration was delayed with respect to the occlusion and mirrored the timeline of the hypertensive response. Vagal blockade eliminated these decelerations in the non-acidemic sheep. Thus, “intermittent placental insufficiency” can cause decelerations and its effects are mediated by the vagus nerve. These “late” decelerations were not associated with fetal acidosis. 1, 3
When the occlusions were extended to produce fetal acidosis, the fetal hypertensive response lost its progressive character, reaching a plateau early after the beginning of the occlusion, while the deceleration continued to fall with its nadir occurring at or after the end of the occlusion. With progressive acidemia the decelerations became deeper and longer. In the presence of very severe acidemia (pH=6.96) they could not be eliminated by vagal blockade. With complete vagal and alpha and beta adrenergic blockade, the decelerations persisted. The fetal heart, devoid of any sympathetic and parasympathetic influences, showed decelerations suggesting that intrinsic myocardial depression was the deceleration mechanism in the presence of severe acidosis and hypoxia.3
Although the individual pathways described above cover the major mechanisms of fetal heart rate decelerations, the actual situation is more complex. Even in the sheep experiments using precisely controlled conditions, consistent fetal heart rate decelerations could not be produced equally in all animals despite 2 hours of repetitive maternal vascular occlusions.3