Maternal Mortality articles have surfaced on many major publications and many continue to investigate it. The New York Times recently released an article titled “What is it like to face dying during childbirth in the richest country in the world in the 21st century?” Their article discusses the efforts being made in discovering the causes of these increasing maternal death rates.
New York Times | By Kim Brooks | Opinion | Nov. 16, 2018
For experts studying the United States’ maternal mortality and injury rates — which are estimated to far surpass those in other developed countries — and for women in labor, the failure to treat mothers as people is neither antiquated nor dystopian, but absolutely pressing.
In September, USA Today published a major investigation into recent efforts to curb maternal death rates. A number of states have assigned panels of experts to review what went wrong in cases where mothers die. This sounds promising. Unfortunately, it hasn’t worked — rates have continued to rise — and the reason is hard to fathom.
“At least 30 states have avoided scrutinizing medical care provided to mothers who died, or they haven’t been studying deaths at all,” the newspaper said. “Instead, many state committees emphasized lifestyle choices and societal ills in their reports on maternal deaths. They weighed in on women smoking too much or getting too fat or on their failure to seek prenatal medical care.” Mothers, it seems, in addition to being held solely responsible for every facet of their child’s well-being, are also being held responsible for their own deaths.
Talk about blaming the victims.
According to USA Today, when asked about their decision not to scrutinize medical care, some doctors on the panels said they didn’t have the resources, and that hospitals don’t like to (and aren’t required to) hand over their dead patients’ charts. Lawmakers claimed that it wasn’t the job of the state to meddle with doctors’ decisions. And state officials argued that it was more important to focus on broader issues surrounding maternal health than on what may have gone wrong in specific women’s cases.
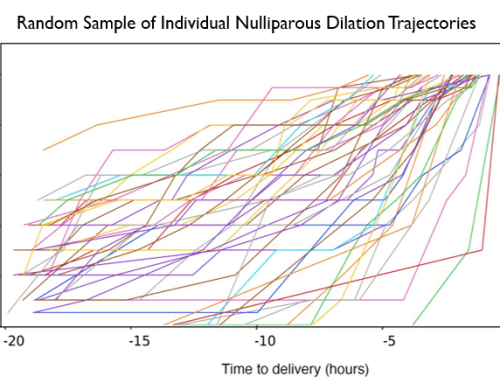
Studies show that 50 percent or more of poor outcomes in childbirth are preventable
The problem isn’t that we don’t know how to make childbirth safer. Stephanie Teleki, who leads the maternity care portfolio at the California Health Care Foundation, put it this way in an interview: “Women know what they want when it comes to labor and delivery, and it turns out the things they want (midwives, doulas, fewer unnecessary interventions and cesarean sections) are less expensive and produce better outcomes.” The problem is not that pregnant women are uneducated or uninformed; the problem is that those in charge aren’t listening to them.
I wanted to know what it is like to experience this — to face one’s death during childbirth in the richest country in the world in the second decade of the 21st century. Obviously, I couldn’t talk to women who had died in childbirth. So I spoke to women who had almost died. That’s what led me to Thea.
After 36 hours of pitocin, a drug that induces labor, and three hours of pushing, Thea required a cesarean because the baby had turned sideways. Prolonged exposure to pitocin can increase the risk of postpartum hemorrhaging. And that’s what happened a few minutes after her daughter was delivered. Thea bled for three hours, while she got intravenous drugs to promote clotting and signed forms in case she ended up needing an emergency hysterectomy.
“They kept telling me how healthy the baby was,” she told me, “but that only made me more terrified that now I might die.” She spent a week in the hospital.
“They did save me in the end,” she says, “but after they almost killed me.”
When Serena Williams spoke out about the medical emergency she endured after the birth of her child last year, and the psychological trauma she suffered as a result, she began a long-overdue debate on America’s abysmal rates of maternal death and injury, as well as the ways that women of color bear the brunt of subpar care.
African-American women are nearly 3.5 times more likely than white women to die from pregnancy-related conditions. “Women are not being listened to,” Dr. Teleki told me. “But black women are the least listened to and it’s costing them their lives at a much higher rate.”
Ms. Williams’s story offered a personal glimpse into an epidemic of preventable deaths that has long been ignored in this country.
In 2000, United Nations member states issued a Millennium Development Goal of, by 2015, cutting the 1990 maternal death ratio by 75 percent. Through a large-scale international effort, maternal mortality was reduced by 43 percent worldwide during that period, and by almost 50 percent in developed countries. Meanwhile, the rates of American women dying from pregnancy rose.
A maternal-fetal early warning system reduces unanticipated NICU usage by 52 percent
The only exception in the United States was California, where, in 2006, the Stanford University School of Medicine worked with the state to create the California Maternal Quality Care Collaborative. The initiative developed “quality improvement tool kits” that doctors and hospitals could download. They included detailed instructions about best practices for various preventable complications that can arise during or after pregnancy, like hemorrhaging and pre-eclampsia.
This sounds simplistic, but it had a powerful effect. “What you have to understand,” Dr. MacDorman explained, “is that these emergencies are horrible and they happen too often, but still, they’re not common. An O.B. might easily go a year without encountering such an emergency.”
As a result of this initiative, between 2006 and 2013, California saw a 55 percent decrease in the maternal mortality rate, from 16.9 to 7.3 deaths for every 100,000 live births. During that same period, according to The Washington Post, the national rate increased — from an estimated 13.3 to 22 deaths in 100,000.
These numbers, disturbing as they are, don’t account for the far greater number of women who are injured during delivery or suffer the trauma of near-death experiences. For many, this trauma can last a lifetime.
Claire, who also asked that I use only her first name, was 38 weeks into her fourth pregnancy in 1992 when she went into the hospital certain she was in active labor. She protested when the doctor decided that the baby wasn’t full-term and gave shots to halt the labor. A few weeks later the baby’s head descended and Claire returned to the hospital, but the baby was now so big that she labored unsuccessfully for 24 hours before undergoing an emergency C-section.
This is how she described her experience: “They gave me an epidural and asked me if I could feel the knife and I said, ‘Yes, I can,’ and they didn’t believe me. They said that’s impossible. But I kept saying, ‘No, I can feel it.’” Then her blood pressure dropped. “I hear my husband say, ‘Look at her blood pressure.’ And the doctor said, ‘Oh, that must be a malfunction of the machine.’ Then I hear, ‘Oh, my God, she’s going into shock,’” she explained. “At one point I heard them say, ‘We’re going to lose her, we’re going to lose the baby’.”
Claire still remembers it as one of the most terrifying experiences of her life. “I never completely got over it,” she told me. “I have a daughter now who’s pregnant. I’d like to just be happy about it but I can’t be.”
Thea’s daughter is now 13. She decided not to tell her how terrible the experience of her birth was, for fear she won’t want to have kids herself.
There was another reason, though, she told me, in a follow-up email to our conversation: “I didn’t want my daughter to know that the joy of her birth was mixed with trauma and the fear of my own death.” She still finds herself feeling guilty for that fear, for “caring about myself and my mortality.” This, she wrote, “speaks to the way I, and probably many other women, was dehumanized and demeaned during the delivery,” and told that “our babies are much more important than we are.”
“I was invested in maintaining that narrative as a way to love her,” Thea wrote.
Kim Brooks (@KA_Brooks) is the author of “Small Animals: Parenthood in the Age of Fear.” Article and images from The New York Times.