by Emily Hamilton, MDCM
Senior Vice President, Clinical Research, PeriGen
“In the New Year, you carry all the experiences of the past years and that is the greatest power of every New Year! This year, you are less student and more master!”
~Mehmet Murat Ildan, Contemporary Novelist & Playwright
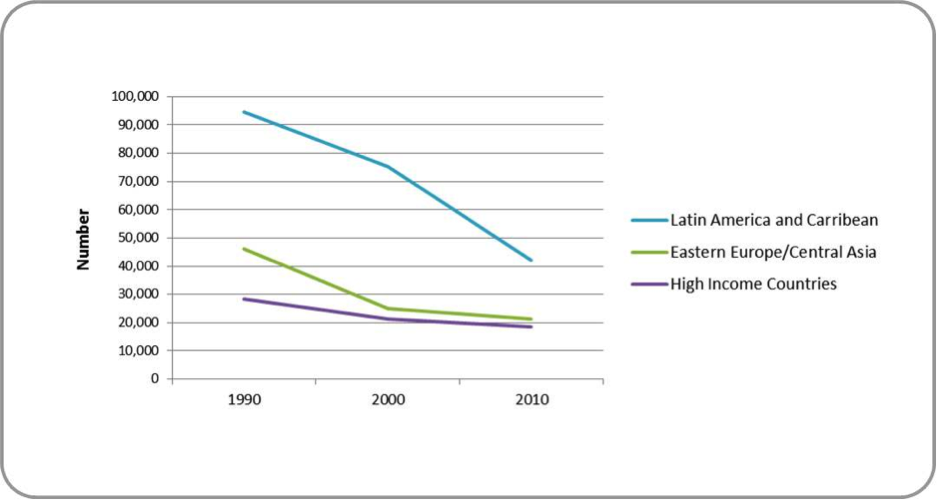
Figure 1. Falling rates of intrapartum-related neonatal encephalopathy
Just as individuals gain experience and wisdom on life’s journey, so do organizations, professions and companies. Experience helps because as professionals we are entrusted with responsibility both at a personal and organizational level to provide safe maternity care. Among the myriad of challenges crying for our attention, which ones are critical, have a chance for success, or bring the greatest benefit for our mothers, babies and their families? With the New Year beginning it is time to pause and reflect on some of the lessons learned and past accomplishments because they will help us plan our journey for the coming year. As you read on, note the clarity of insights gained by using “Big Data” and “Wide Lenses” for time and geography.
One of the United Nation’s Millennium Goals – to reduce child mortality, has brought us more reliable data on an important obstetrical topic: namely, intrapartum-related neonatal encephalopathy (IP-NE). On a world scale, intrapartum-related hypoxic events are estimated to have a huge impact – contributing to ¼ of neonatal deaths and ½ of late pregnancy stillbirths. They make the largest single-condition contribution to disability adjusted life-years. 1-4
When one examines progress over 20 years in multiple countries, steady incremental improvement is evident. Figure 1 shows the falling rates of IP-NE in regions including and most similar to the US1 Rates in all the other geographical regions were much higher. They all showed progressive descent fell except for the region of Sub-Saharan Africa.
Two other recent and large studies provide further important insights regarding the nature of IP-NE and related clinical care. 5, 6 Researchers in Sweden, where infant mortality rates are generally amongst the best in the world, examined 71,189 birth records to investigate the association between EFM patterns and neonatal outcome. 5 The rates of neonatal encephalopathy were very low at 1.1 per 1000 births. They concluded that moderate and severe encephalopathy was attributable to asphyxia in 60% of their NE cases and most evolved during labor.
Moving closer to home, Clark et al examined the effect of compliance vs non-compliance with an oxytocin administration protocol in 14,398 women undergoing induction of labor at HCA.6 Oxytocin misuse is a common finding in births with severe metabolic acidosis. 7-9 Furthermore, oxytocin misuse is a modifiable risk factor. In this most recent study compliance was associated with:
- Fewer admissions to the NICU (3.8% vs 5.2% P=0.01)
- Fewer low Apgar scores (4.9% vs 6.4% P=0.04)
- Fewer cesareans (15.8% vs 18.8% P<0.01)

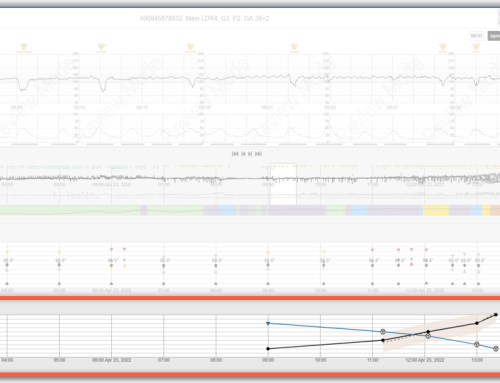
Figure 2. PeriCALM Patterns display showing the analysis related to uterine tachysystole
Members of our own PeriGen family have experienced similar success stories. 10 MedStar Franklin Square Medical Center launched a highly successful IT initiative focusing on uterine tachysystole (overly frequent contractions). PeriCALM Patterns fetal monitoring software with built-in pattern recognition and specialized long-term graphical displays was introduced in 2011. At a glance any clinician could detect if uterine tachysystole (UT) was present, if it was transient or persistent, if it provoked fetal heart rate decelerations and see the Montevideo units as is shown in Figure 2.
This study involved the systematic re-examination of each 30-minute segment of tracing from all 10,518 monitored term labors. Comparing years before immediately before and after the introduction of PeriCALM Patterns they observed that:
- The rate of UT with oxytocin fell from 22.7% to 17.3% P<0.0001.
- Average duration of UT fell from 64 minutes to 54 minutes.
- Total time spent in UT fell by 36.5%.
Long term trends analysis is a key component of helping humans see significant trends and to anticipate what is about to happen. In psychological parlance this ability to assess current conditions and project the most likely development is known as situational awareness. In medical behavioral studies it is one of the key skills required across all acute care settings.
Computers are masters of rapid computation and efficient data visualization. Anecdotes from nursing staff related how the displays made easy it was to see when uterine tachysystole was present or even about to occur. Continuous calculations removed the subjectivity of choosing where to count the contraction rates. Quantitative data facilitated communication because predominant patterns were clearly evident. Nurses had the authority to stop oxytocin when uterine tachysystole occurred.
There is abundant evidence today that the human brain has a fixed functional capacity and that every mental task we perform detracts from our ability to do another at the same time. 11 Computers are very consistent at number crunching, that is counting, adding, measuring or doing exactly what they are programmed to do. In contrast, humans are very good at reasoning based on deep clinical understanding Clinicians will always have to integrate EFM tracing findings with other clinical information. That said, the repetitive analytic capacity of PeriCALM Patterns and its long-term displays are useful adjuncts for clinicians. This study demonstrated the synergistic effects of this technology and dedicated clinicians. Together they achieved an impressive reduction in UT.
In summary, what lessons have we learned?
Lesson 1. It is impossible to see progress in rare conditions using small samples over short periods of time. Rates derived from large data sets and trends over long periods are much more revealing.
Lesson #2. A substantial portion of NE arises and evolves during labor.
Lesson #3. The incidence of intrapartum-related NE, a devastatingly serious condition, is falling.
Lesson #4. Clinical actions matter. Oxytocin protocol compliance is associated with better neonatal condition and lower cesarean rates. Uterine tachysystole rates can be reduced.
Lesson #5. Computers and clinicians can be highly synergistic.
No one is suggesting that technology replace clinicians. However, computerization is useful for tasks like calculations, data visualization, reminders and communication thus freeing clinicians to focus applies their energy on higher level reasoning and clinical interventions.
Maternal child health care has come a very long way. Detractors of EFM often refer to randomized clinical trials conducted more than 30 ago that showed no neonatal survival benefit with EFM, although EFM use was associated with a substantial reduction in the incidence of neonatal seizures. In the largest of these studies, deaths or seizures occurred at an astonishing rate of 1 in 225.12 Today, intrapartum fetal death is exceedingly rare and moderate and severe IP-NE are estimated to occur in approximately 1.5/1000 births among the High-Income countries and 0.6/1000 specifically in the Swedish study. This achievement did not happen by chance. Concerted efforts on many fronts have contributed. It happened in part, because most clinicians did not adopt a defeatist attitude such as believing that the origins of IP-NE were beyond our influence or that EFM held no value. Rather these clinicians continued to find better ways to fine tune the imperfect tools that are available and improve our health care systems.
Healthcare informatics has also evolved. We have seen a maturation of software for basic hospital wide electronic medical records and convergence on a few products. With this accomplishment we have seen an increasing demand for the efficient overlay of smart modules with real clinical benefits. In parallel, the PeriGen experience has confirmed our belief that the most useful smart software applications are those that harness the power of computers to do what they do best especially in areas that humans find challenging or time consuming.
As for the New Year, we will continue to apply sound analytical methods on high impact clinical issues where objective quantitative analysis helps clinicians see critical factors or developing trends and intervene in a timely fashion. We have reached a new level in medical informatics and a very exciting one indeed. Stay tuned as we work to bring these ideas to the bedside.
References
1. Lee AC, Kozuki N, Blencowe H, Vos T, Bahalim A, Darmstadt GL, Niermeyer S, Ellis M, Robertson NJ, Cousens S, Lawn JE. Intrapartum-related neonatal encephalopathy incidence and impairment at regional and global levels for 2010 with trends from 1990. Pediatr Res. 2013 Dec;74 Suppl 1:50-72. doi: 10.1038/pr.2013.206.
2. Wn J, Shibuya K, Stein C. No cry at birth: global estimates of intrapartum stillbirths and intrapartum-related neonatal deaths. Bull World Health Organ. 2005 Jun;83(6):409-17. Epub 2005 Jun 17.
3. Lawn JE, Lee AC, Kinney M, Sibley L, Carlo WA, Paul VK, Pattinson R, Darmstadt GL. Two million intrapartum-related stillbirths and neonatal deaths: where, why, and what can be done? Int J Gynaecol Obstet. 2009 Oct;107 Suppl 1:S5-18, S19. doi: 10.1016/j.ijgo.2009.07.016
4. Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet. 1997 May 17;349(9063):1436-42.
5. Jonsson M, Agren J, Nordén-Lindeberg S, Ohlin A, Hanson U. Neonatal encephalopathy and the association to asphyxia in labor. Am J Obstet Gynecol. 2014 Dec;211(6):667.e1-8. doi: 10.1016/j.ajog.2014.06.027. Epub 2014 Jun 17.
6. Clark SL, Meyers JA, Frye DK, Garthwaite T, Lee AJ, Perlin JB. Recognition and response to electronic fetal heart rate patterns – impact on newborn outcomes and primary cesarean delivery rate in women undergoing induction of labor. Am J Obstet Gynecol. 2014 Nov 22. pii: S0002-9378(14)02249-2. doi: 10.1016/j.ajog.2014.11.019. [Epub ahead of print]
7. Clark SL, Belfort MA, Dildy GA, Meyers JA. Reducing obstetric litigation through alterations in practice patterns. Obstet Gynecol. 2008 Dec;112(6):1279-1283.
8. Berglund S, Grunewald C, Pettersson H, Cnattingius S. Severe asphyxia due to delivery-related malpractice in Sweden 1990-2005. BJOG. 2008 Feb;115(3):316-323.
Jonsson M, Nordén SL, Hanson U. Analysis of malpractice claims with a focus on oxytocin use in labour. Acta Obstet Gynecol Scand. 2007;86(3):315-319.
10. Smith S, Bunting K, Hamilton E. Using Intelligent Electronic Fetal Monitoring Software to Reduce Iatrogenic Complications of Childbirth: A Case Study.J Healthc Inf Manag, in press
10. Rock D., Your Brain at Work: Strategies for Overcoming Distraction, Regaining Focus, and Working Smarter All Day Long Harper Business. Harper Collins, New York, NY.
12. MacDonald D, Grant A, Sheridan-Pereira M, Boylan P, Chalmers I. The Dublin randomized controlled trial of intrapartum fetal heart rate monitoring. Am J Obstet Gynecol. 1985 Jul 1;152(5):524-39